Understanding Lewy Body Dementia
Lewy Body Dementia (LBD) is a complex and often misunderstood brain disorder. It’s a progressive condition, meaning symptoms worsen over time, and it affects both mental abilities and movement. Unlike Alzheimer’s disease, which primarily impacts memory, or Parkinson’s disease, which is largely defined by movement issues, LBD presents a unique combination of cognitive and motor symptoms.
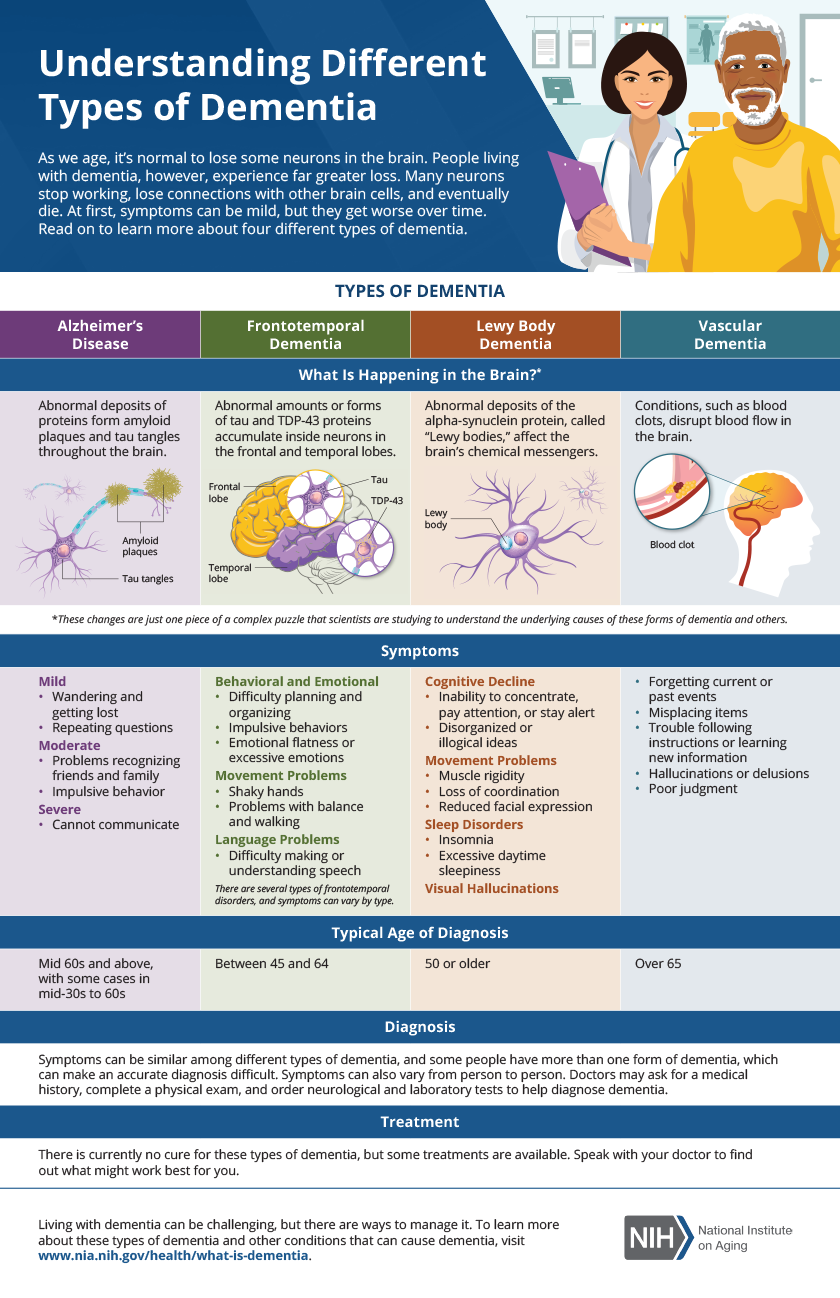
LBD is caused by abnormal deposits of a protein called alpha-synuclein, known as Lewy bodies, in the brain. These deposits disrupt brain function, leading to a wide range of symptoms. The exact reason why these deposits form isn't fully understood, and families should recognize that research is ongoing.
LBD is frequently misdiagnosed because its symptoms overlap with other conditions, and the fluctuating nature of cognitive abilities can confuse doctors. LBD is the second most common type of progressive dementia after Alzheimer’s, accounting for 10-25% of dementia cases, yet many people go years without a correct diagnosis. This delay hinders access to appropriate care and support.
LBD symptoms vary significantly but generally fall into three main categories: cognitive changes, motor symptoms, and behavioral and psychological symptoms. Recognizing these categories helps in understanding the disease and navigating its challenges. LBD impacts everyone differently, and its progression is highly individual.
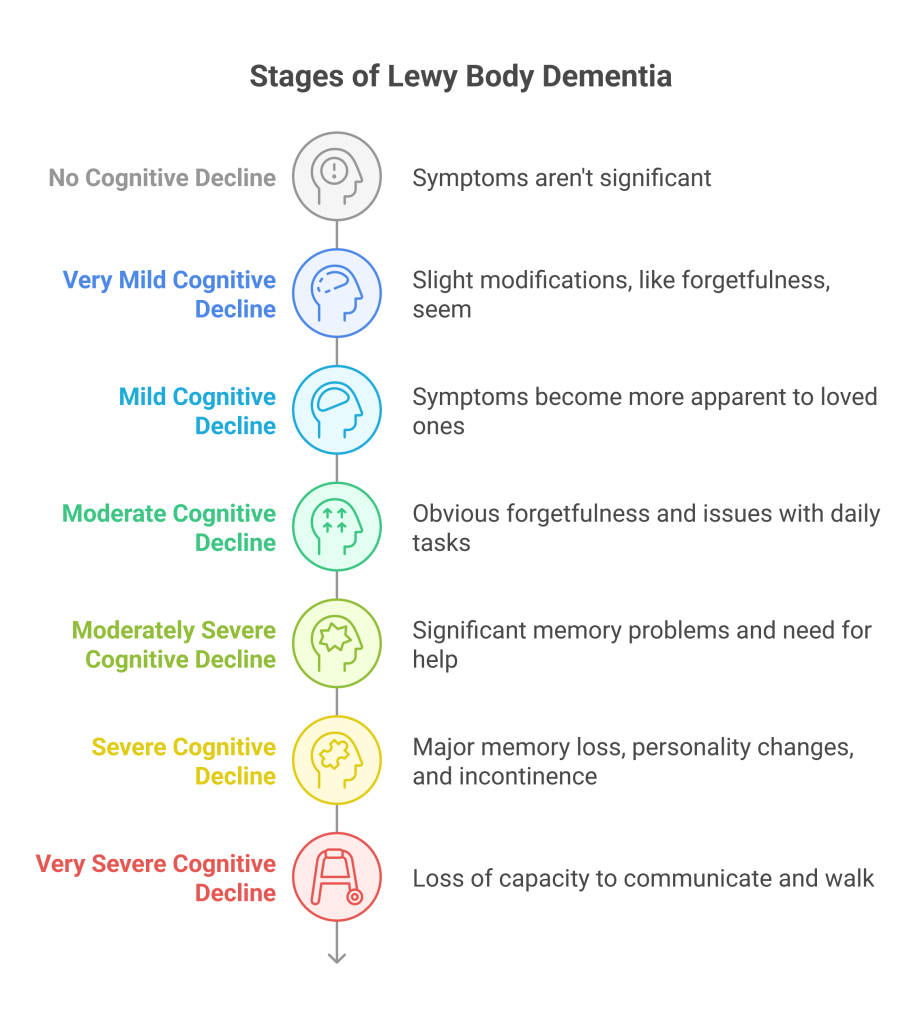
The Seven Stages: A Detailed Breakdown
The Lewy Body Dementia Resource Center outlines seven stages of LBD, providing a framework for understanding the disease’s progression. These stages aren’t rigid timelines; individuals may move through them at different rates, and some may experience symptoms out of sequence. The stages offer a useful guide for families and caregivers.
Stage 1: Very Mild Cognitive Changes. In the earliest stage, changes are subtle and may not be readily apparent. Individuals might experience mild memory problems, such as occasionally misplacing items or forgetting appointments. There might also be subtle changes in personality or mood. Motor symptoms are typically absent or very mild.
Stage 2: Mild Cognitive Decline. Cognitive difficulties become more noticeable. Individuals may struggle with concentration, experience difficulty finding the right words, or have problems with visual-spatial skills. Motor symptoms, such as mild tremor or stiffness, may begin to emerge. Fluctuations in alertness and attention are often present.
Stage 3: Mild to Moderate Cognitive Decline. This stage marks a more significant decline in cognitive abilities. Individuals may have difficulty with complex tasks, such as managing finances or following conversations. Visual hallucinations, often of people or animals, become more common. Motor symptoms, like slowness of movement and postural instability, are more pronounced.
Stage 4: Moderate Cognitive Decline. Cognitive impairment is now clearly evident, impacting daily life. Individuals may experience confusion, disorientation, and difficulty with memory. Hallucinations and delusions are frequent. Motor symptoms, including rigidity and gait disturbances, interfere with mobility. Assistance with daily activities is often needed.
Stage 5: Moderate to Severe Cognitive Decline. Individuals experience significant cognitive impairment and require substantial assistance with daily living. Communication becomes increasingly difficult, and hallucinations and delusions may be more intense. Motor symptoms are severe, leading to falls and increased dependence.
Stage 6: Severe Cognitive Decline. Individuals have profound cognitive impairment and require full-time care. They may be unable to recognize family members or communicate effectively. Motor symptoms are debilitating, and they often experience difficulty swallowing.
Stage 7: End Stage. This is the final stage of LBD, characterized by complete dependence on others for all aspects of care. Individuals are often bedridden and unable to respond to their environment. The focus shifts to providing comfort and managing symptoms. The average life expectancy after diagnosis is between 5 and 8 years, but this varies greatly.
- Stage 1: Very mild cognitive changes (Symptoms may be subtle and easily dismissed)
- Stage 2: Mild Cognitive Decline (Difficulty with concentration and word-finding)
- Stage 3: Mild to Moderate Cognitive Decline (Visual hallucinations become more common)
- Stage 4: Moderate Cognitive Decline (Significant impact on daily life)
- Stage 5: Moderate to Severe Cognitive Decline (Substantial assistance needed)
- Stage 6: Severe Cognitive Decline (Full-time care required)
- Stage 7: End Stage (Complete dependence and focus on comfort)
Stages of Lewy Body Dementia: A Quick Reference
| Stage Number | Cognitive Symptoms | Motor Symptoms | Behavioral/Psychiatric Symptoms | Typical Duration |
|---|---|---|---|---|
| 1 | Mild cognitive decline; problems with concentration, executive function, and visual-spatial abilities. May experience fluctuating alertness and attention. | Mild motor symptoms, such as slight tremor or rigidity, may begin. | Possible mild depression, anxiety, or apathy. | Variable, often several years. |
| 2 | Increasing difficulties with attention, concentration, and problem-solving. Memory impairment becomes more noticeable. | Motor symptoms become more apparent, potentially including slowed movement, rigidity, and postural instability. | Fluctuations in alertness and attention become more pronounced; visual hallucinations may start. | 1-3 years |
| 3 | More significant cognitive impairment affecting daily functioning. Difficulty with planning, organization, and multitasking. | Balance problems and gait disturbances become more frequent, increasing risk of falls. Tremor may be present. | Visual hallucinations become more frequent and complex. Delusions may also occur. Behavioral disturbances like agitation can emerge. | 1-3 years |
| 4 | Moderate to severe cognitive decline. Significant memory loss and confusion. Difficulty with language and communication. | Motor symptoms worsen, potentially leading to a parkinsonian-like state with rigidity, bradykinesia (slowness of movement), and postural instability. | Hallucinations and delusions are common. Significant fluctuations in cognitive function and alertness. May experience REM sleep behavior disorder. | Variable, often 1-2 years. |
| 5 | Severe cognitive impairment. Significant difficulty with all aspects of daily living. Loss of recognition of family and friends. | Motor impairments are pronounced, leading to significant disability. Increased risk of falls and injuries. | Severe behavioral and psychiatric symptoms, including agitation, aggression, and psychosis. Communication is severely limited. | 6 months - 2 years |
| 6 | Profound cognitive impairment. Loss of most cognitive abilities. Requires total assistance with daily living. | Severe motor impairment. May become bedridden or chair-bound. Difficulty swallowing. | Behavioral and psychiatric symptoms may continue, but often fluctuate with overall decline. Reduced responsiveness. | Variable, months to a year. |
| 7 | End-stage dementia. Complete loss of cognitive and physical function. Unable to communicate or recognize surroundings. | Severe physical decline. Complete dependence on others for all care. | Minimal responsiveness. Primarily focused on physical comfort. | Weeks to months |
Illustrative comparison based on the article research brief. Verify current pricing, limits, and product details in the official docs before relying on it.
Early Stage Challenges & Support
Stages 1 and 2 of LBD present challenges because symptoms are often subtle and attributed to normal aging or other conditions, leading to delayed diagnosis. Mild memory lapses, difficulty finding the right words, and subtle personality changes can be dismissed as simply "having a senior moment."
Motor symptoms in the early stages might include a mild tremor, stiffness, or slowness of movement. These symptoms can be mistaken for early Parkinson’s disease, especially if cognitive changes are not yet apparent. Fluctuating cognition – periods of clarity followed by confusion – is a hallmark of LBD but can be easily overlooked or misinterpreted.
If you are concerned about a loved one, seek a thorough medical evaluation. A geriatrician, neurologist, or psychiatrist with experience in dementia is best equipped to diagnose LBD. Provide a detailed history of symptoms, including when they started and how they have progressed. Having a family member present to share observations can be helpful.
Questions to ask the doctor include: "What other conditions could be causing these symptoms?’ ‘What tests will be performed to confirm a diagnosis?’ and ‘What are the treatment options available?" Support groups can also be invaluable during this time, providing a space to connect with others facing similar challenges and learn coping strategies. The Lewy Body Dementia Association (LBDA) offers resources and support groups both online and in person.
Mid-Stage Shifts: Increasing Needs
Stages 3 and 4 of LBD represent a significant shift in the disease’s progression. Cognitive impairment becomes more pronounced, impacting daily life in substantial ways. Individuals may struggle with tasks they previously handled with ease, such as managing finances, preparing meals, or following conversations.
Hallucinations and delusions become more frequent and vivid during this phase. These experiences can be frightening for the individual and distressing for family members. These are symptoms of the disease, not reflections of the person’s underlying reality. Behavioral changes, such as paranoia and agitation, are also common.
Motor symptoms continue to worsen, leading to increased difficulty with mobility and balance. Falls become more frequent, and assistance with activities of daily living (ADLs) – such as bathing, dressing, and eating – is often required. The increasing need for assistance burdens caregivers.
This is often a time of great emotional strain for families. Caregivers may experience grief, frustration, and exhaustion. Prioritize self-care and seek support from friends, family, or a professional counselor. Respite care – temporary relief for caregivers – can provide a break.
- Increased difficulty with daily tasks (finances, cooking)
- More frequent and vivid hallucinations and delusions
- Worsening motor symptoms and increased risk of falls
- Greater need for assistance with activities of daily living
Late-Stage Care: Comfort and Dignity
Stages 5, 6, and 7 of LBD involve profound cognitive and physical decline. Individuals require full-time care and are often unable to communicate effectively or recognize loved ones. Care focus shifts from maintaining independence to providing comfort and ensuring dignity.
Managing pain and other physical symptoms is paramount. Individuals may experience difficulty swallowing, leading to malnutrition and aspiration pneumonia. Attention to nutrition and hydration is essential. Regular medical evaluations can help address underlying medical conditions contributing to discomfort.
As the disease progresses, end-of-life considerations become important. Palliative care can provide symptom management and emotional support for the individual and their family. Hospice care offers comprehensive end-of-life care, including medical, emotional, and spiritual support.
Even in the late stages of LBD, individuals deserve respect and compassion. Maintaining a calm and peaceful environment, providing gentle touch, and playing familiar music can provide comfort and reassurance. The goal is to ensure their final days are as comfortable and dignified as possible.
Medication & Therapies: Current Approaches
There is currently no cure for Lewy Body Dementia, and treatment focuses on managing symptoms. Medications are available to address cognitive impairment, motor symptoms, and behavioral disturbances. Cholinesterase inhibitors, such as donepezil and rivastigmine, may help improve cognitive function in some individuals. However, they can also cause side effects, such as nausea and diarrhea.
Medications to manage motor symptoms, such as levodopa, may be prescribed, but they can sometimes worsen hallucinations. Antipsychotics may be used to control hallucinations and delusions, but they carry a risk of serious side effects and should be used with caution. It's important to have a detailed conversation with a doctor about the risks and benefits of any medication.
Non-pharmacological therapies, such as physical therapy, occupational therapy, and speech therapy, can also play a valuable role in managing symptoms. Physical therapy can help maintain mobility and prevent falls. Occupational therapy can help individuals adapt to their changing abilities and maintain independence. Speech therapy can address communication difficulties.
Research into new treatments for LBD is ongoing, and there is hope that more effective therapies will be developed in the future. Clinical trials are an important avenue for exploring new treatment options. The Lewy Body Dementia Association (LBDA) provides information about current clinical trials.
- Cholinesterase inhibitors (donepezil, rivastigmine) for cognitive symptoms
- Levodopa for motor symptoms
- Antipsychotics (use with caution) for hallucinations and delusions
- Physical, occupational, and speech therapy
Resources & Support Networks
Navigating a Lewy Body Dementia diagnosis can feel overwhelming, but support is available. The Lewy Body Dementia Association (LBDA) is dedicated to improving the lives of people affected by LBD. Their website offers educational materials, support groups, and a helpline.
The National Institute on Aging (NIA) also provides valuable information about LBD on their website (). This resource offers a comprehensive overview of the disease, including its causes, symptoms, and diagnosis.
Local support groups can provide a safe and supportive environment to connect with others facing similar challenges. Respite care services can offer caregivers a much-needed break from their responsibilities. Many communities also offer adult day care programs, which can provide social and recreational activities for individuals with LBD.
Remember, seeking help is a sign of strength, not weakness. By connecting with resources and support networks, you can empower yourself and your loved one to navigate the challenges of LBD with greater confidence and resilience.
- Lewy Body Dementia Association (LBDA):
- National Institute on Aging (NIA):
- Local support groups: Check with the LBDA or NIA for resources in your area
- Respite care services: Contact your local Area Agency on Aging


No comments yet. Be the first to share your thoughts!