Understanding Lewy Body Dementia
Lewy Body Dementia, or LBD, is a complex and often misunderstood condition. It’s a progressive type of dementia, meaning the symptoms worsen over time, and it accounts for an estimated 10-25% of all dementia cases. What sets LBD apart is the presence of abnormal protein deposits, called Lewy bodies, in the brain. These deposits disrupt brain function, leading to a variety of cognitive, behavioral, and movement-related symptoms.
Lewy bodies are made of a protein called alpha-synuclein. In LBD, this protein misfolds and clumps, disrupting how brain cells communicate. LBD isn't one disease but a spectrum of disorders with similar features, making diagnosis difficult.
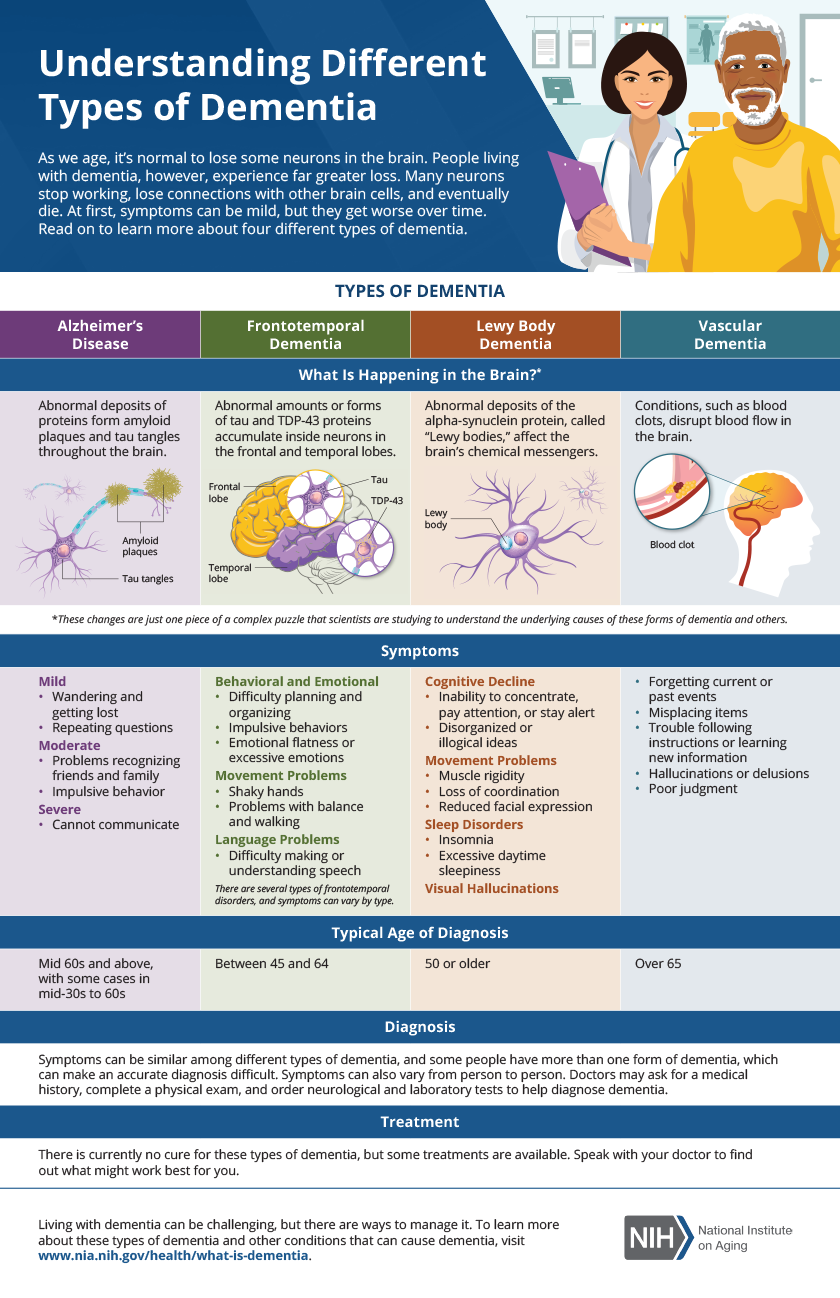
LBD is frequently confused with Alzheimer’s disease and Parkinson’s disease, and even can present similarly to both. Unlike Alzheimer’s, which primarily affects memory early on, LBD often begins with fluctuations in alertness and attention, visual hallucinations, and problems with movement. While Parkinson’s also involves movement difficulties, the cognitive symptoms and hallucinations are more prominent and occur earlier in LBD. Because of these overlapping symptoms, LBD is often misdiagnosed, highlighting the need for increased awareness and specialized diagnostic tools.

The 7 stages of Lewy body dementia
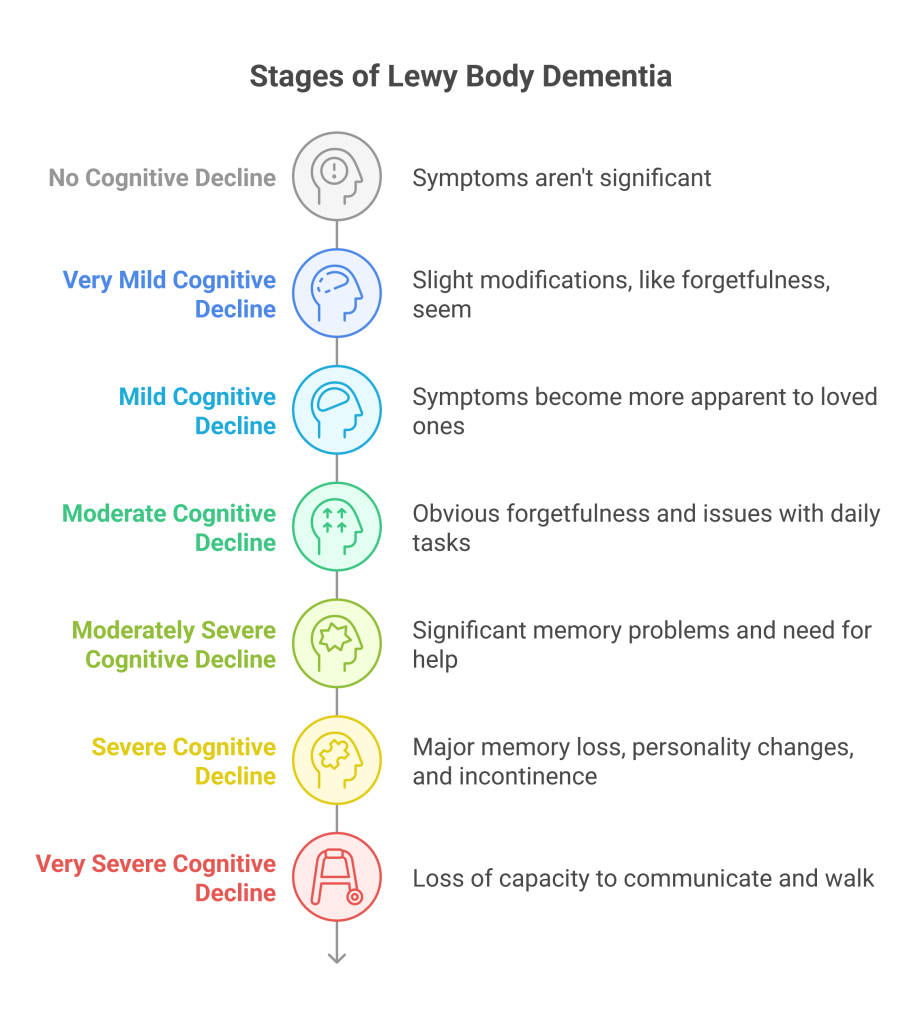
The Lewy Body Dementia Resource Center outlines 7 stages to help understand the disease's progression. These stages aren't rigid; individuals experience LBD differently, and progression isn't always linear. Someone might spend more time in one stage than another, or experience symptoms out of sequence. This framework offers a guide for caregivers and medical professionals.
Stage 1: Very Mild Cognitive Changes. In the earliest stage, changes are subtle and may not be immediately noticeable. A person might experience mild difficulties with concentration, slight personality changes, or mild depression. These changes are often attributed to normal aging, making diagnosis difficult. You might notice a loved one seeming a bit more withdrawn or less interested in activities they once enjoyed.
Stage 2: Mild Cognitive Decline. At this stage, cognitive difficulties become more apparent. Problems with attention and executive function – planning, organizing, and problem-solving – start to emerge. Difficulty following conversations, repeating questions, and needing help with familiar tasks become common. Sleep disturbances, like restless legs syndrome or REM sleep behavior disorder (acting out dreams), often begin in this stage, sometimes years before other symptoms.
Stage 3: Mild to Moderate Cognitive Decline. This is where fluctuations in cognition become more pronounced. A person may have periods of clarity interspersed with periods of confusion or disorientation. Visual hallucinations, often of people or animals, may begin. Motor symptoms, such as stiffness, slowness, or tremors, might also start to appear, but are usually less prominent than in Parkinson’s disease. It’s common for individuals to misinterpret what they see, which can be frightening for them.
Stage 4: Moderate Cognitive Decline. Cognitive impairment is now significant and impacts daily life. Hallucinations become more frequent and vivid. Problems with movement worsen, leading to difficulties with walking and balance. Fluctuations in alertness and attention are more pronounced, and a person may experience periods of profound confusion. They’ll likely require increased assistance with daily tasks like dressing and bathing.
Stage 5: Moderate to Severe Cognitive Decline. This stage marks a significant decline in cognitive abilities. The person experiences frequent and prolonged periods of confusion, disorientation, and hallucinations. Motor symptoms become more severe, often requiring the use of a walker or wheelchair. Communication becomes increasingly difficult, and they may struggle to recognize familiar faces. According to the National Institute on Aging, managing medications is a significant challenge at this stage due to sensitivity to side effects.
Stage 6 & 7: Severe Cognitive Decline. These final stages involve profound cognitive and physical decline. The person is largely unresponsive, requires total care, and may be unable to communicate. Hallucinations and delusions may persist. The focus of care shifts to providing comfort, managing pain, and ensuring dignity. Palliative care is essential during this time.
Early stage challenges
Stages 1 and 2 are arguably the most challenging to recognize, both for the individual experiencing them and for their loved ones. The symptoms are often subtle and can be easily dismissed as normal aging, stress, or mild depression. This delay in diagnosis can be detrimental, as early intervention can potentially slow the progression of the disease and improve quality of life.
Look for changes in personality – a normally outgoing person becoming more withdrawn, or a typically calm person becoming irritable. Pay attention to sleep patterns; REM sleep behavior disorder, where a person physically acts out their dreams, is a strong indicator of LBD and often precedes other symptoms by years. Subtle changes in sense of smell have also been noted in some cases.
The anxiety felt by caregivers during these early stages is understandable. You sense something isn't quite right, but you can’t put your finger on it. It's important to trust your instincts and seek a thorough medical evaluation, including a neurological assessment. Don’t hesitate to advocate for your loved one and request specialized testing for LBD.
Mid-stage complications
Stages 3-5 of LBD are characterized by more prominent and disruptive symptoms. Visual hallucinations become increasingly common, often involving detailed and realistic scenes. These aren’t simply fleeting images; they can be complex and involve interactions with perceived individuals or objects. It's crucial to remember that the person experiencing the hallucination believes it is real.
Responding to hallucinations requires a calm and reassuring approach. Avoid arguing with the person or trying to convince them that what they’re seeing isn’t real. Instead, acknowledge their experience and offer comfort. For example, you might say, “That sounds frightening,” or “I’m here with you.”
Movement problems, like rigidity, slowness, and postural instability, also become more noticeable. This can increase the risk of falls, making home safety modifications essential. Remove tripping hazards, install grab bars in the bathroom, and ensure adequate lighting. Managing medication can be complex, as individuals with LBD are often sensitive to side effects. Work closely with a neurologist to find the right balance of medications to manage symptoms without causing undue distress.
Fluctuating cognition is a hallmark of LBD during these stages. A person may be alert and oriented one moment, and confused and disoriented the next. This unpredictability can be incredibly challenging for caregivers. Establish a consistent routine and provide a calm, structured environment to minimize confusion.
- Remove tripping hazards (rugs, cords)
- Install grab bars in bathrooms
- Ensure adequate lighting throughout the home
Late-stage care
Stages 6 and 7 of LBD require a significant shift in focus. The primary goal is to provide comfort, manage pain, and ensure the person’s dignity. Cognitive abilities are severely impaired, and communication is limited. Palliative care becomes essential, focusing on relieving suffering and improving quality of life.
Caregivers need to prioritize self-care during this challenging time. The emotional and physical demands of providing 24/7 care can be overwhelming. Respite care – temporary relief for caregivers – is crucial for preventing burnout. Support groups offer a valuable opportunity to connect with others who understand the challenges of LBD.
End-of-life planning is also important. Discuss the person’s wishes regarding medical treatment, and ensure that legal documents, such as a healthcare proxy and advance directive, are in place. Remember that even when a person is no longer able to communicate, their comfort and dignity remain paramount.
New research
Research into LBD is ongoing, and while there is currently no cure, several promising areas of investigation are emerging. Studies are focused on identifying potential biomarkers for early detection, which could allow for earlier intervention. Researchers at the National Institute on Aging are exploring the role of alpha-synuclein in the development of LBD and are investigating potential therapies to prevent its misfolding and aggregation.
Clinical trials are underway to evaluate the effectiveness of existing medications, as well as new drugs specifically designed to target the underlying pathology of LBD. While results are still preliminary, some studies suggest that certain medications may help to manage symptoms such as hallucinations and motor problems. However, it's important to approach these findings with caution, as more research is needed to confirm their benefits.
Non-pharmacological interventions, such as cognitive stimulation therapy and exercise programs, are also being investigated as potential ways to improve cognitive function and quality of life in people with LBD. These therapies aim to engage the brain and promote neuroplasticity, the brain’s ability to adapt and reorganize itself.
Resources and support
Navigating LBD can feel isolating, but numerous resources are available to provide support and guidance. The Lewy Body Dementia Association (LBDA) () offers a wealth of information, including educational materials, support groups, and a helpline. The National Institute on Aging (NIA) () provides research updates and fact sheets on LBD.
Local support groups can offer a valuable opportunity to connect with other caregivers and share experiences. Online forums and communities also provide a platform for sharing information and seeking advice. Remember, you are not alone in this journey.

No comments yet. Be the first to share your thoughts!