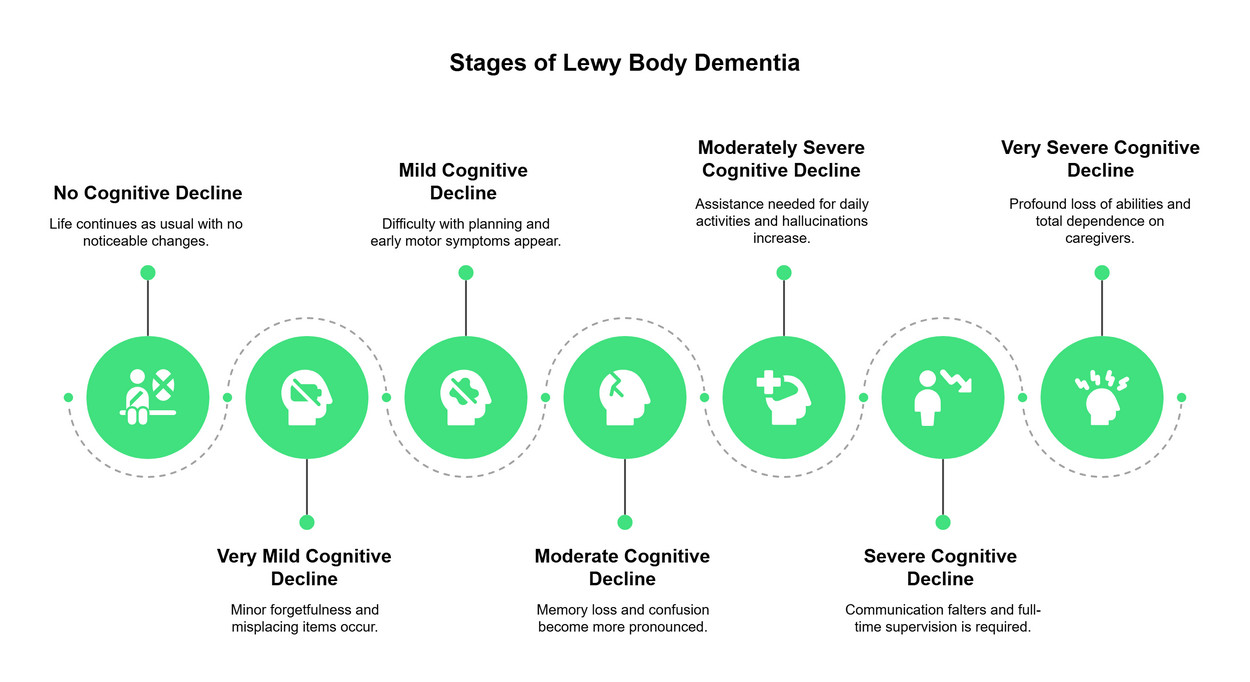
7 Stages of Lewy Body Dementia: A Caregiver’s Timeline
Lewy body dementia progresses through seven distinct stages, each marked by specific cognitive and physical changes. This timeline outlines what to expect as the condition evolves, helping you anticipate needs and plan care effectively.
What Lewy Body Dementia Looks Like
Lewy body dementia (LBD) is a complex brain disorder that affects thinking, movement, and behavior. Unlike other dementias that primarily impact memory first, LBD often begins with visual hallucinations, sleep disturbances, and fluctuations in alertness. This makes the early signs difficult to recognize and diagnose.
The seven-stage framework provides a roadmap for families navigating this journey. It helps caregivers anticipate changes in cognition, physical ability, and independence. However, LBD progression is rarely linear. Some individuals move through stages quickly, while others remain in one stage for years. This unpredictability is a defining feature of the disease.
Understanding these stages does not mean predicting a fixed outcome. Instead, it offers a way to prepare for the shifting needs of your loved one. By recognizing the pattern of decline, families can adjust care plans, manage symptoms, and maintain quality of life for as long as possible.
Adjusting care as stages progress
Lewy body dementia follows a predictable trajectory, but the rate of decline varies. Caregivers must shift their approach at each transition to maintain safety and dignity. What works in the early stages fails as cognitive and physical abilities change. This timeline outlines how to adjust care strategies as the disease advances.
Stage 1-2: Early adjustments
In the initial stages, independence is still possible but requires subtle support. Focus on establishing routines that reduce confusion. Use calendars, labeled cabinets, and consistent meal times. Safety checks are minimal but necessary; ensure medications are organized and driving assessments are discussed early. Communication remains clear, so involve the person in care decisions while they still have capacity.
Stage 3-4: Increasing supervision
As memory loss and visual hallucinations become more frequent, supervision must increase. Remove hazards that were previously manageable, such as loose rugs or unsecured chemicals. Address safety concerns directly but calmly. Introduce assistive devices like walkers or grab bars if mobility issues appear. Communication may become repetitive; respond with patience rather than correction. Begin planning for long-term care needs, including legal and financial arrangements.
Stage 5-6: Comprehensive support
Significant cognitive decline requires round-the-clock support. Daily activities like bathing and dressing become challenging. Establish a consistent daily routine to reduce anxiety. Monitor for worsening hallucinations or paranoia, which may require medical intervention. Safety risks escalate; ensure the home is secure against wandering. Nutrition and hydration become critical concerns. Consider professional in-home care or memory care facilities if family caregiving becomes unsustainable.
Stage 7: End-of-life care
In the final stage, the person is largely nonverbal and requires full physical assistance. Focus on comfort, pain management, and dignity. Palliative care specialists can help manage symptoms like seizures or severe agitation. Communication shifts to nonverbal cues; gentle touch and a calm presence are most effective. Hospice care may be appropriate to support both the person and the family through this difficult transition.
Common Questions About LBD Stages
Work through to the 7 Stages of Lewy Body Dementia


No comments yet. Be the first to share your thoughts!