7 Stages of Lewy Body Dementia: Care Strategies and Family Support
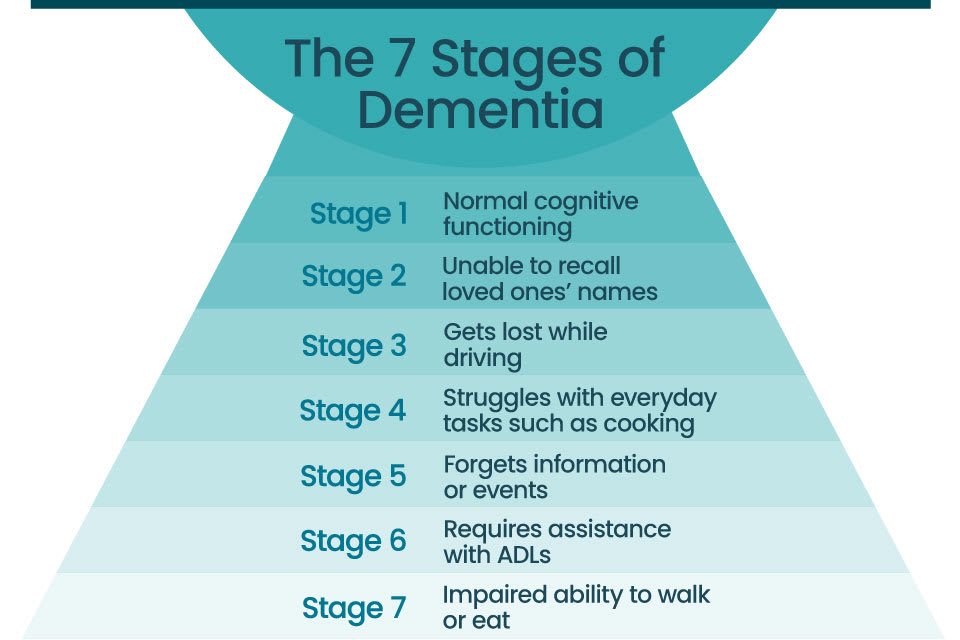
Lewy body dementia progresses through seven distinct stages, each bringing unique challenges for patients and caregivers. Understanding this timeline helps families anticipate needs and adjust care strategies effectively.
-

Early stage cognitive fluctuations and subtle memory changes
Patients experience sudden shifts in alertness, often described as staring into space or having moments of unavailability. Memory lapses appear mild, with word-finding difficulties and trouble recalling recent events. Caregivers should document these variations to distinguish them from normal aging, establishing a baseline for future medical discussions and adjusting daily expectations accordingly. -
00314-X/asset/d0d96c02-a259-4a34-b76c-96c184483f36/main.assets/gr1_lrg.jpg)
Emerging visual hallucinations and mild motor symptoms
Distinct visual hallucinations of people or animals often emerge, sometimes causing fear or confusion. Mild motor signs like stiffness or a shuffling gait may appear alongside these perceptual changes. Families should avoid arguing about the reality of these visions, instead offering calm reassurance and checking the environment for triggers like poor lighting or shadows that exacerbate misinterpretations. -
Progressive parkinsonism and increased sleep disturbances
Motor symptoms worsen significantly, resembling Parkinson’s disease with tremors, rigidity, and balance issues. Sleep patterns deteriorate, often involving REM sleep behavior disorder where patients physically act out dreams. Safety modifications become essential, including removing tripping hazards and installing bed rails. Medical management focuses on balancing motor symptom relief without worsening cognitive function or causing excessive sedation. -

Severe cognitive decline and frequent delusions
Cognitive abilities deteriorate further, leading to an inability to recognize familiar faces or understand simple commands. Delusions become more fixed and distressing, such as believing caregivers are imposters. Communication shifts to non-verbal cues, requiring patience and gentle touch. Caregivers must prioritize emotional comfort over factual correction, creating a calm environment that minimizes agitation and confusion during interactions. -

Physical rigidity and difficulty with daily tasks
Severe physical immobility sets in, often requiring full assistance for movement, eating, and hygiene. Swallowing difficulties may develop, increasing the risk of aspiration pneumonia. Care transitions toward palliative support, focusing on dignity, pain management, and comfort. Family members should prepare for end-of-life discussions, ensuring care preferences align with the patient’s values while managing the physical burdens of advanced disease progression. -

Loss of speech and complete dependence on care
As language centers deteriorate, verbal communication often ceases, leaving patients nonverbal and entirely reliant on others for all daily needs. Caregivers must learn to interpret nonverbal cues like facial expressions or gestures to identify pain, hunger, or discomfort. This stage requires constant supervision to prevent falls and manage complex medical needs, shifting the dynamic from assisted living to intensive, around-the-clock support for basic survival functions. -
End-stage complications and palliative care needs
The final phase involves severe physical decline, including difficulty swallowing, increased susceptibility to infections like pneumonia, and total immobility. Medical focus shifts from disease modification to comfort, emphasizing pain management, hygiene, and emotional presence for the patient and family. Palliative care teams help navigate these complex decisions, ensuring dignity and minimizing suffering as the body’s systems gradually shut down, requiring compassionate end-of-life support.
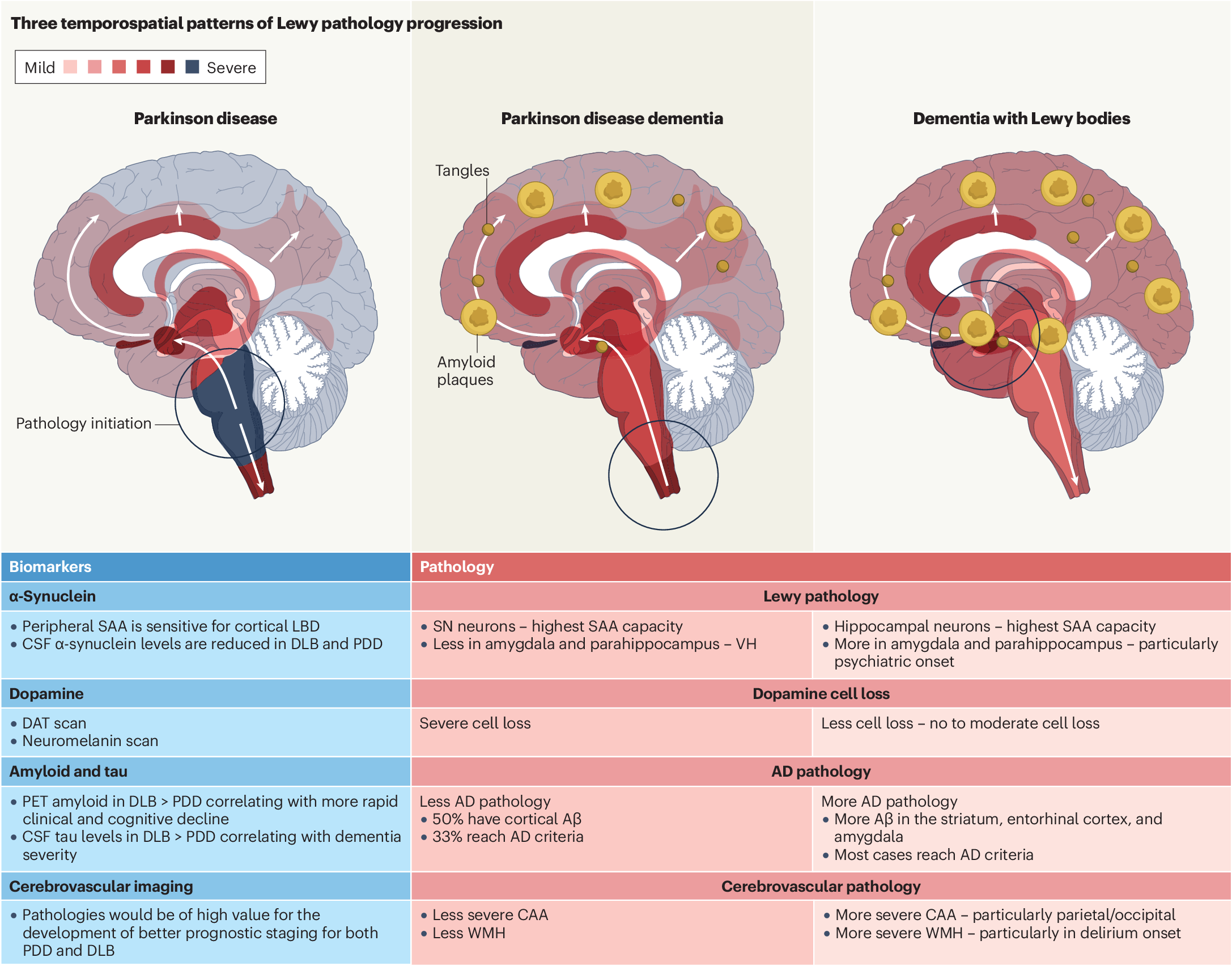
What defines Lewy body dementia
Lewy body dementia (LBD) is a progressive disease that causes a gradual decline in mental abilities. It is the second most common type of dementia after Alzheimer’s disease, accounting for an estimated 10% to 20% of all dementia cases.
Unlike Alzheimer’s, which primarily targets memory first, LBD affects movement, thinking, and behavior simultaneously. This happens because of abnormal protein deposits called Lewy bodies in the brain. These deposits disrupt the brain's chemical balance, leading to a unique mix of symptoms.
Visual hallucinations are a core feature. Many people with LBD see detailed images of people or animals that aren't there. These visions often appear early in the disease course, whereas in Alzheimer’s, they typically occur only in later stages.
Motor issues also set LBD apart. Symptoms can resemble Parkinson’s disease, including stiffness, tremors, slow movement, and balance problems. Sleep disturbances are another hallmark; many patients experience REM sleep behavior disorder, acting out vivid dreams physically.
Cognitive fluctuations are common. A person with LBD might be alert and clear-headed one hour, then confused and drowsy the next. This variability can make daily planning difficult for families.
Understanding these distinct symptoms helps families recognize LBD early. Proper diagnosis ensures access to specific care strategies and support resources tailored to this complex condition.
Subtle changes and early signs
The first stage of Lewy body dementia often looks like normal aging. Memory slips happen, but they rarely stop daily life. People might forget names or misplace keys. They may struggle to find the right word. These changes are mild and easy to dismiss.
Vision problems often appear before memory loss. Objects might look blurry or distorted. Depth perception can fail, making stairs tricky. Simple tasks like pouring coffee become harder. These visual issues are early warnings of Lewy body dementia, not just eye strain.
Sleep changes are another common early sign. People may talk, yell, or thrash in their sleep. This is often REM sleep behavior disorder. It happens years before other symptoms. The brain is not properly paralyzing muscles during dreams.
Mood swings and anxiety can start early. A person might become unusually worried or depressed. They may lose interest in hobbies. These emotional shifts are part of the disease process. They are not just "getting old."
Caregivers should watch for these subtle signs. Early detection helps with planning and support. It allows families to adjust before things get worse. Keeping a journal of changes can help doctors.
Stage 2: Mild Cognitive Impairment
Stage 2 is often the first time family members notice something is different. The person can still function independently, but memory lapses and executive function issues become visible. This phase is characterized by subtle changes in daily tasks rather than a complete loss of ability.
Common signs include forgetting familiar words, losing items in unusual places, or having trouble with complex planning. A person might struggle to balance a checkbook or follow a multi-step recipe. These errors are not due to normal aging but signal that the brain is starting to struggle with processing speed and recall.
While the individual remains capable of self-care, they may need more time to complete tasks that used to be automatic. Family members often step in to help with logistics, such as managing appointments or organizing finances. This support helps maintain independence while reducing stress for the person with Lewy body dementia.
The Mayo Clinic notes that dementia refers to a wide range of symptoms affecting a person's ability to perform everyday activities independently. In this stage, that independence is still largely intact, but the foundation is shifting. Recognizing these early signs allows families to plan for future care needs without rushing into dependency.
Stage 3: Moderate Dementia Begins
Stage 3 marks a shift from mild confusion to significant cognitive decline. People with Lewy body dementia (LBD) often experience a noticeable worsening of memory and thinking skills. Daily tasks that were once simple, like managing finances or following a recipe, become challenging. This stage requires more consistent support and supervision to maintain safety and independence.
Hallucinations are a hallmark of this stage. Visual hallucinations—seeing people, animals, or objects that aren’t there—affect up to 80% of individuals with LBD. These visions are usually detailed and vivid. Unlike the vague shadows seen in other dementias, LBD hallucinations can feel very real. Family members should avoid arguing about the reality of these sights. Instead, validate the person’s feelings and gently redirect their attention to a calming activity.
Sleep disturbances often emerge or worsen during moderate dementia. REM sleep behavior disorder (RBD) is common, where the normal muscle paralysis of REM sleep fails. This causes patients to physically act out their dreams, sometimes violently. They may shout, punch, or fall out of bed. This stage requires safety-proofing the bedroom, such as removing sharp objects or placing padding on the floor, to prevent injury.
The combination of cognitive decline and physical sleep disruptions can be exhausting for both the patient and caregivers. Establishing a strict bedtime routine and ensuring a safe sleep environment are essential first steps. Professional medical evaluation can help manage these symptoms with medication if necessary.

Stage 4: Moderate to Severe Decline
By this stage, Lewy body dementia has progressed significantly. The person needs daily assistance with basic activities like dressing, bathing, and eating. Simple tasks that were manageable in earlier stages now require step-by-step guidance or full support from a caregiver.
Motor symptoms become more pronounced. Stiffness and rigidity in the limbs increase, making movements slow and difficult. These physical changes often resemble Parkinson’s disease, leading to shuffling walks and a higher risk of falls. The brain’s ability to process physical signals slows down, requiring a safer home environment.
Confusion and cognitive decline deepen. The person may struggle to recognize family members or remember recent events. Hallucinations and delusions often become more frequent and distressing during this phase. Clear, simple communication helps reduce anxiety, while consistent routines provide a sense of stability.
Caregivers must shift from supportive oversight to active management. This includes monitoring medication effects, managing behavioral changes, and ensuring physical safety. The National Institute on Aging notes that these changes require a structured care plan to maintain quality of life for both the patient and their family.
Stage 5 severe dementia needs help
Use this section to make the 7 Stages of Lewy Body Dementia decision easier to compare in real life, not just on paper. Start with the reader's actual constraint, then separate must-have requirements from details that are merely nice to have. A practical choice should survive normal use, maintenance, timing, and budget. If a recommendation only works in an ideal situation, call that out plainly and give the reader a fallback path.
The simplest way to use this section is to write down the must-have criteria first, then compare each option against those criteria before weighing nice-to-have features.
Stage 6: Very Severe End-Stage Care
By stage 6, Lewy body dementia has progressed to a point where basic physical abilities are largely lost. Individuals often require round-the-clock care for all activities of daily living. They may lose the ability to speak coherently, relying on single words or phrases to communicate needs and emotions. Mobility declines significantly, making walking difficult or impossible without assistance.
Physical symptoms become the primary focus of care. Incontinence is common, requiring regular hygiene management to prevent skin breakdown and infection. Swallowing difficulties (dysphagia) increase the risk of choking and aspiration pneumonia, which is a leading cause of death in this stage. Caregivers must adapt meal preparation to safe textures, such as pureed foods or thickened liquids, to ensure safe nutrition and hydration.
The emphasis shifts entirely to palliative and comfort-focused care. The goal is no longer to reverse decline but to maintain dignity and minimize distress. This involves managing pain, agitation, and sleep disturbances with careful medical oversight. Regular repositioning helps prevent pressure ulcers, and gentle touch or familiar music can provide comfort when verbal communication is no longer possible.
Supporting the patient and family during this phase requires a team approach. Healthcare providers, hospice services, and family members collaborate to ensure the patient’s comfort. The World Health Organization notes that dementia care at this stage focuses on improving quality of life and supporting the well-being of caregivers who face immense emotional and physical burdens. Open communication about care goals and advance directives becomes essential for making decisions that align with the patient’s values.
Practical care strategies for families
Managing Lewy body dementia (LBD) requires a different approach than other dementias. The symptoms fluctuate daily, and the brain’s sensitivity to medications creates unique challenges. Caregivers must adapt their strategies to address hallucinations, motor issues, and medication sensitivities without causing distress.
Step 1: Manage hallucinations with calm reassurance
Hallucinations are common in LBD and can be frightening for both the patient and the caregiver. Instead of arguing about what is real, validate the person’s feelings. If they see someone in the room, ask if they feel unsafe, then gently reassure them you are there. Do not try to correct the hallucination with logic, as this often increases agitation. Keep the environment calm and well-lit to reduce shadows that might trigger visual distortions.
Step 2: Adjust medications carefully
People with LBD are extremely sensitive to antipsychotic medications. Standard drugs used for confusion or agitation in other dementias can cause severe, sometimes irreversible, side effects in LBD patients, including rigid muscles and loss of mobility. Always consult a neurologist or geriatric psychiatrist before starting any new medication. Regular medication reviews help reduce polypharmacy, which often worsens confusion and motor symptoms.
Step 3: Support movement and safety
Motor symptoms like stiffness, shuffling gait, and balance problems increase fall risk. Simple safety modifications can prevent injury. Remove loose rugs, install grab bars in bathrooms, and use non-slip mats. Encourage gentle, regular movement like walking or seated exercises to maintain flexibility. If the person has Parkinsonism, allow extra time for them to initiate movement, as they may experience "freezing" episodes where they feel stuck in place.
Step 4: Improve communication techniques
Communication difficulties often arise from cognitive fluctuations. Speak in short, simple sentences and give one instruction at a time. Use non-verbal cues like gentle touch or pointing to reinforce your message. If the person becomes confused or agitated, pause and try again later. Maintaining a consistent routine helps reduce anxiety and provides a sense of security.
-
Safety-proof the home: remove tripping hazards and install grab bars
-
Review all medications with a doctor to avoid sensitive antipsychotics
-
Establish a consistent daily routine to reduce confusion
-
Practice calm reassurance during hallucinations without arguing
These strategies focus on safety, comfort, and maintaining dignity. By adjusting to the unique needs of LBD, families can provide more effective support during this challenging journey.
Frequently asked questions about Lewy body dementia
How fast does Lewy body dementia progress? Lewy body dementia (LBD) is a progressive condition, meaning symptoms worsen over time. Progression varies significantly between individuals. Some people experience a steady decline over several years, while others may have periods of stability followed by rapid changes. On average, life expectancy after diagnosis is 5 to 7 years, though some live up to 20 years depending on overall health and care quality.
Can Lewy body dementia be cured? There is currently no cure for Lewy body dementia. Treatment focuses on managing symptoms and improving quality of life. Medications can help control cognitive issues, movement problems, and psychiatric symptoms like hallucinations. Non-drug approaches, such as physical therapy and speech therapy, also play a vital role in maintaining function and independence for as long as possible.
How is Lewy body dementia diagnosed? Diagnosing LBD is complex because symptoms overlap with Alzheimer’s disease and Parkinson’s disease. Doctors rely on a detailed medical history, physical and neurological exams, and cognitive tests. There is no single blood test or scan that confirms LBD. Diagnosis often involves ruling out other conditions and looking for specific signs, such as visual hallucinations or fluctuating alertness, which are hallmarks of the disease.
What are the early signs of Lewy body dementia? Early symptoms often include visual hallucinations, sleep disturbances like acting out dreams (REM sleep behavior disorder), and subtle cognitive changes. Memory loss may not be the first sign, unlike in Alzheimer’s. Instead, patients might experience confusion, attention problems, or difficulty planning tasks. Movement symptoms similar to Parkinson’s disease, such as stiffness or slow movement, may also appear early.
Is Lewy body dementia hereditary? Most cases of Lewy body dementia are not directly inherited. While family history can play a role, LBD is generally considered sporadic. However, having a close relative with LBD or Alzheimer’s disease may slightly increase your risk. Genetic factors are being studied, but no single gene causes the disease in most people.
How does Lewy body dementia differ from Alzheimer’s disease? While both are types of dementia, LBD often presents with visual hallucinations, fluctuating cognition, and movement issues earlier in the disease course. Alzheimer’s typically begins with memory loss and progresses to language and spatial problems. LBD also involves sensitivity to antipsychotic medications, which can cause severe side effects in LBD patients but are less problematic in Alzheimer’s patients.
Work through to the 7 Stages of Lewy Body Dementia



No comments yet. Be the first to share your thoughts!